» Introduction
» Trismus
» Purpose of Physiotherapy
» Procedure of Physiotherapy / Chemotherapy
» Appliances
» Case Reports (patients)
» Salient Features
» Conclusion
» Important notes on Shekar's Appliance
» Fabrication of the Appliances
» Videos
» Statement
Temporomandibular joints-TM Joints- in the human body are the most exclusive ones which are also called as diarthodial joints because of their unique features. Each of the osseous components of TM Joint articulate with an interposed fibrous connective tissue disc. This arrangement permits a range of motion unique to this joint. TMJ functions as a double joint-with different types of movements in various directions and also the right and left jointshave to work in unison.
The TMJ is one of the complex joints in the human body as it provides hinge(ginglimo) movements in one place and sliding (arthrodial) movements at the same time. Hence it is technically called as Ginglymoarthrodial Joint. TMJ differs from other diarthrosis, as it does not have cartilaginous tissue covering the opposing joint surface. This joint has a layer of fibrous connective tissue overlying the articular surface.
The uniqueness of this joint does not limit only to its anatomical, histological and functional aspects, but the disorders of this joints are also unique and as complicated as the joint is.
Etiology of these disorders may occur even during birth (forceps delivery) or at any time later in the life span of the individual. The factors may be local like trauma, ear infection, improper co-ordination between the Condylar head and articular disc movements and malocclusion. Commonly it occurs due to inflammation and spasm of the muscles due to operative trauma including birth injuries to the TMJ (Forceps delivery). It can also occur due to infection of the spaces like Pterygomandibular space, submassetric space, and other systemic diseases like juvenile arthritis, rheumatoid and osteoarthritis etc..
Trismus refers to patient’s inability to open the mouth to normal extent. In most of the pathologically involved TMJ disorders, there will be a gradual reduction in the degree of mouth opening leading to Trismus, commonly called as lockjaw.
Trismus can occur at an early age whenever there is injury or infection of the TMJ resulting in fibrous ankylosis initially and bony ankylosis at a later stage. This in turn interferes with the normal growth and development of TMJ, the mandible and the associated structures. These developmental disturbances of the TMJ compounded by trismus results in the development of the handicapping malocclusion and dentofacial deformity.
In treating these cases, the practical physiology of functional development has to be applied so as to improve the movements of the TM joints and to bring about the normal growth and development of the complete stomatognathic system. This can restore the physical, physiological, social and psychological well being of a person in the society.
Till now, surgery is considered to be the choice of treatment for TMJ ankylosis. But in majority of the cases ankylosis recur after surgery. Hence even though surgery is successful, rehabilitation makes the difference between success and failure of the treatment. Most of the physiotherapeutic appliances which have been in use till now, are not in accordance with the biological principles of growth and development and physiological functioning of the stomatognathic system. This appliance which works according to biological principles has been successfully tried in treating the cases of trismus due to various etiological factor
Face is not only the index of mind but also can be the index of health and personality of an individual. In that, oral cavity is the most important organ from where functioning of the digestive system begins. Mouth is also an organ of smile which is unique to the human beings provided one can open the mouth. If there is any difficulty or decreased in opening of the mouth then it is called TRISMUS.
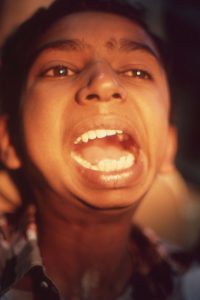
Trismus is a pathological condition where the patient cannot open the mouth to normal extent. It is also called as restricted mouth opening. This restriction can be complete where the mouth cannot be opened at all as in case of bony ankylosis of Temporomandibular Joint, or it can be partial where, the mouth opening is possible to some extent as in case of oral sub mucous fibrosis and such other conditions. In majority of the cases trismus occurs due to spasm or stiffness of the masticatory muscles and mucous membrane resulting in restriction of the jaw movements.(fig.1)

(Fig-1)
Hans Heinz Naumann et al (Differential diagnosis in otorhinolaryngology; Hans Heinz Naumann, Frank Martin, Karin Schoris; 1993, published by Thieme) have studied the degree of mouth opening in cases of trismus and they have given different grades depending upon the extent of opening.
Grade 1 – opening ranging from 2.5 to 4 cm
Grade 2 – opening ranging from 1 to 2.5 cm
Grade 3 – less than 1 cm
And Total trismus (Complete) – is the situation where the patient cannot move the mandible.
Normal mouth opening in adults is 50.9 mm in males and 47.1 mm in females.
The etiology of trismus is varied in nature. The spasm of the muscles or the inflammation of the temporomandibular joint can occur due to any of the following factors:
The trismus can be called as temporary or partial where the mouth can be opened to some extent in cases like impacted 3rd molars, post surgical complications and such other conditions. In case of temporary or partial trismus, the disease can be treated successfully in a short period of time depending upon the etiology . There are no deleterious effects on the growth, development and functioning of the stomatognathic system. The disease can be successfully treated with chemotherapy along with physiotherapy by which the trismus is released and the normal functioning of the system can be restored.
In case of total trismus mouth opening is almost nil, particularly so in case of bony ankylosis of the Temporomandibular Joint. Manifestations of TMJ ankylosis is not just trismus but it also affects the growth, development and functions of the stomatognathic system resulting in HANDICAPPING MALOCCLUSION AND DENTOFACIAL DEFORMITY.(fig.2)

(Fig-2)
This kind of ankylosis can occur in children due to various reasons such as birth injuries- forceps delivery, juvenile arthritis and trauma. In these cases the growth and development of both soft and hard tissues will be affected resulting in retarded growth of the affected structures. This lack of growth and development of affected structures results in lack of functioning of these structures. In turn, lack of function result in lack of growth and development of the affected structures.
Let us know some more about this unique joint of the human body- TEMPOROMANDIBULAR JOINT
Temporomandibular joints-TM Joints- in the human body are the most exclusive ones which are also called as diarthrodial joints because of their unique features. Each of the osseous components of TM Joint articulate with an interposed fibrous connective tissue disc. This arrangement permits a range of motion unique to this joint. TMJ functions as a double joint-with different types of movements in various directions and also the right and left joints have to work in unison.
The TMJ is one of the complex joints in the human body as it provides hinge (ginglimo) movements in one plane and sliding (arthrodial) movements at the same time. Hence it is technically called as Ginglymoarthrodial joint. TMJ differs from other diarthrosis, as it does not have cartilaginous tissue covering the opposing joint surfaces. This joint has a layer of fibrous connective tissue overlying the articular surfaces.
The uniqueness of this joint does not limit only to its anatomical, histological and functional aspects, but the disorders of this joint are also unique and as complicated as the joint is.
Here is a clinical manifestation which requires a treatment approach which not only needs treatment for trismus but also has to induce the growth and development of affected structures in the most natural way, as per the biological principles of growth and development. In case of ankylosis of TM joint, depending upon whether it is unilateral or bilateral, the development of mandible is reduced and deformed to a greater extent along with the associated structures. In case of unilateral ankylosis the growth of the structures on the affected side is reduced where as it is normal on unaffected side. This results in facial deformity and severe malocclusion along with the trismus (Fig 3).

(Fig-3)
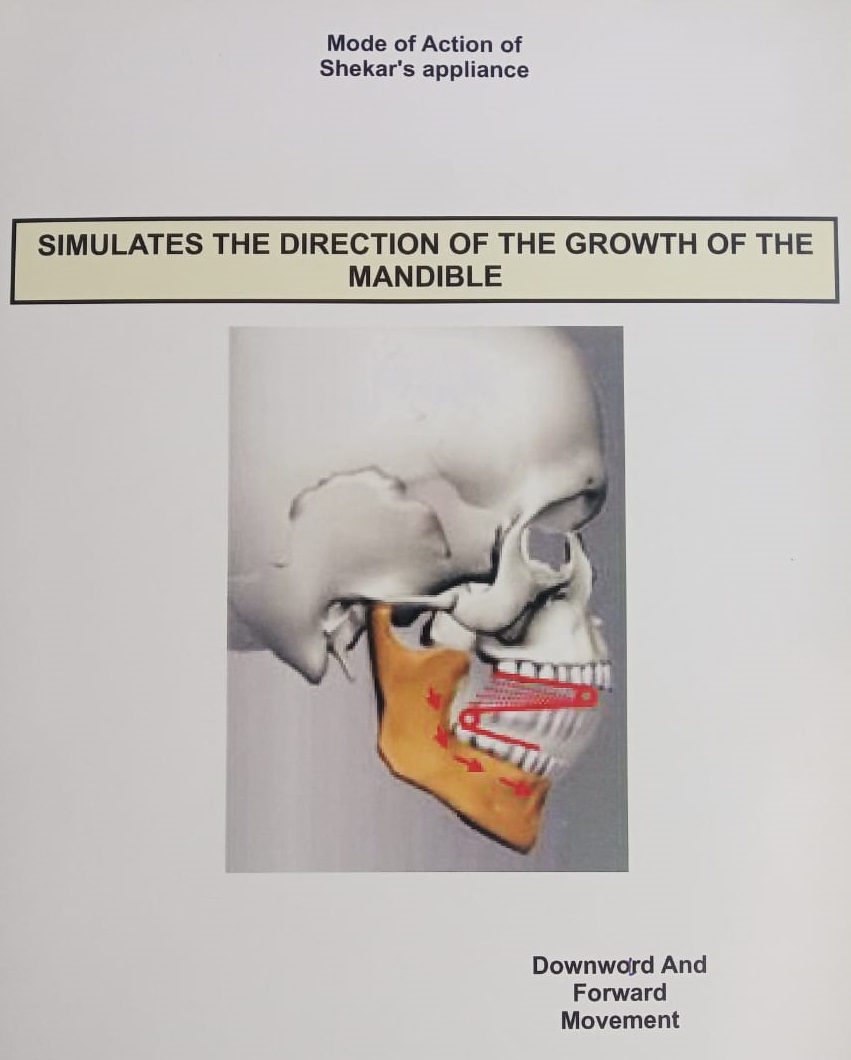
Hence any treatment procedures, whether it is surgical or nonsurgical depending upon the etiology should be followed by physiotherapeutic rehabilitation along with the necessary chemotherapy. Since we are treating growing children, it is very much important to induce the growth and development of the affected structures as much as possible in the natural way and in natural direction. Since the mandible grows in the downward and forward direction, we should also try to induce the growth and development by the functional means (physiotherapeutic aid) in the same direction as per the natural growth. Hence there is a need for an appliance (or physiotherapeutic aids) which not only brings about opening of the mouth (releasing trismus) but also induces the growth and development by repeated function or movement of the mandible along with associated structures in downward and forward direction simulating normal growth and development of the mandible.
Till now surgery is considered to be the treatment of choice of TMJ ankylosis. But in some cases ankylosis recur after sometime. Hence even though the surgery is successful, rehabilitation makes the difference between success and failure of the treatment.
Most of the physiotherapeutic aids which have been used till now have only one purpose to achieve that is opening of the mouth – in the vertical direction. Some of the physiotherapeutic aids which are used are mouth prop, wooden screws, tongue blades and similar appliances (Fig 4). But in these appliances the force applied is-

(Fig-4)
These appliances do help in treating trismus (i.e., mouth opening) for short duration, like post extraction trismus. But in cases where there is a need not only to open the mouth but also to regain or induce the lost growth and development of structures, there is the need to apply the forces in such a way that it should bring about the growth and development of the affected structures back to the normal direction by functional means. Hence there is an absolute need for the application of force on the mandible of the affected patients in the downward and forward directions as well as to rotate in the clockwise direction
To overcome the above said problems, a new appliance was designed and fabricated incorporating springs which can bring about opening of the mouth by exerting a downward and forward pressure on the mandible with the support of the maxillary dental arch. This appliance because of the spring action brings about distraction and contraction of the musculature which involves whole of the stomatognathic system, thus inducing functional development of the mandible and associated structures which are a biological process. The mandible acquires not only vertical but also lateral and rotatory movements. The springs are designed in such a way that their direction of movement is in line with the direction of opening movement of the mandible which is downward and forward.


Procedure of physiotherapy depends upon the etiology of trismus, age of the patient and nature of trismus. Basically it involves selection (making) of proper size appliance with proper gauge of the wire. Frequency of activation of the springs and duration of wearing of the appliance depends upon the etiology and nature of the patient. Generally springs are activated once a week.
Medication – whenever it is required like antibiotics, (in cases of surgical intervention). Analgesics anti-inflammatory fibrolytic drugs and muscle relaxants are given depending upon the need.
Appliance is worn most of the time during the day for the first 2-3 days in case of bony ankylosis, (after surgical intervention, fibrous ankylosis, submucous fibrosis, osteoarthritis. Later it can be worn 5-6 times a day depending upon the need. patient is asked to keep the appliance in the mouth as shown in the picture (video) and hold the handle firm and do the exercise by closing and opening the mouth to the maximum extent till the patient feel pain/fatigue of the masticatory muscles. Treatment in children may be continued for longer period(1-2years) depending upon the growth and development of mandible and associated structures of the stomatognathic system. Pressure applied varies from 800 to 3000gm.
The distance between the maxillary and the mandibular plates can be increased or decreased either by opening the side coils or by closing them – respectively. If the maxillary (Upper) coil is opened (activated) the appliance exerts more pressure on the posterior part of the mandible and if the mandibular (lower) coil is opened (activated) it exerts pressure more on the anterior part of the mandible in clockwise direction. To exert pressure uniformly on the mandible both the coils can be activated bilaterally to the desired extent.
When the patient wears the appliance, the plates will be resting or placed over the occlusal surface of the posterior teeth; it should not touch the anteriors, especially the incisors. For this reason the patient is made to hold the appliance in position and then asked to do the exercises by opening and closing of mouth. Exercises can be done 3 – 4 times a day or even more depending upon the etiology and nature of trismus.
In case of post-extraction trismus recovery can be observed in 1-2 days, whereas in case of osteoarthritis of TMJ, activation may be required after a week for 1 – 2 months. In case of sub mucous fibrosis activation may be required once in 2 – 4 weeks for a longer period of time (6 months – 1 year) depending upon the degree of fibrosis. In case of surgical intervention of the bony ankylosis, activation may be required once a week for 2 – 3 months. In cases of retarded growth of the mandible as in cases of fibrous ankylosis of TMJ, the growth of the mandible can be regained and also directed as per need, by proper activation of the springs and using this appliance for a longer period of 1 – 2 years. This appliance exerts forces on most of the muscles, of the stomatognathic system as well as the neck.
This appliance has been used successfully in the management of following types of pathological lesions resulting in trismus –
As an orthodontist who is interested in the movement of the teeth, I also started working on how to move the mandible and not just opening of the mouth. Patients have to move the mandible not only in vertical direction but also in all other directions as well. As the patients are in the growing age period, I also considered the directions of application of force on the mandible so that the growth can be induced in the downward and forward directions as well as rotation in clockwise direction. The functional development takes place when there is a repeated movement of the mandible with the repeated action of the associated structures. When the appliance is kept in the mouth, patient must be able to open the mouth in downward and forward direction and must also be able to rotate in clockwise direction. But the patient cannot keep the mouth open for a longer period as the muscles cannot be stretched for a long time, hence he will be forced to close the mouth (with the appliance in the mouth). Here also the patient cannot keep the mouth closed for a long time as prolonged contraction of muscles causes’ pain and hence the patient is forced to open the mouth. The patient will be made to close and open the mouth repeatedly in an automatic manner when the appliance is in the mouth.
By considering the physical needs and the biological requirements of physiotherapy in treating the patients with oral trismus, a new appliance was designed incorporating springs which can bring about distraction and contraction of the musculature which is a biological process. The springs were designed in such a way that their direction of movement is in line with the direction of the opening movements of the mandible.
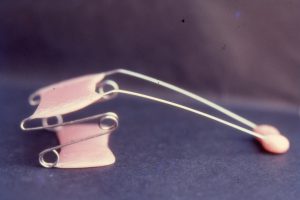
The original appliance fig 5 and 6 consists of maxillary and mandibular full cap splints connected on either side by springs. Splints are prepared on the mounted models related to each other in open mouth position.


This open mouth position is registered by placing the impression compound bungs between upper and lower teeth – when the fibrous ankylosis cases undergo forcible opening under general anaesthesia and when the bony ankylosis cases undergo surgical correction. During the construction of the splints hooks are incorporated in the region of canine and 1st molar in permanent dentition and canine and 2nd molar in deciduous dentition.
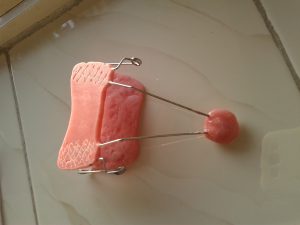
The mechanism of construction and activation of this appliance is a complicated procedure and it is also difficult for the patient to wear as well as to remove the appliance. Hence a modification of this appliance was done so as to make it easy to construct and activate accurately. It will be easy for the patient to wear and do the exercises by keeping in the proper position. This modified appliance consists of two acrylic plates – maxillary and mandibular connected on either side by springs which are incorporated in the acrylic plates. Maxillary acrylic plate is slightly larger than the mandibular acrylic plate. The maxillary plate has a handle connected to it for the patient to hold the appliance in the mouth. The springs are made of 0.9 mm to 1.2 mm stainless steel wire depending upon the nature of trismus and age of the patient. The upper portion of the spring is extended further by about 8.0 cm to make the handle as shown in the fig.
Appliance-2 Followed by –Appliance

Models mounted with the help of compound bungs :

Appliance-1
Front View :
Lateral View :
Front Right view :
Top side wiew :

Lateral View :

Mode Of Action Spring
(For initial opening only)
Spring Compressed :

Spring released :

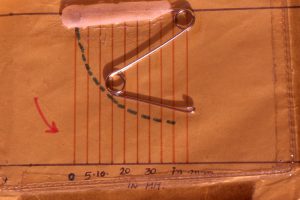
Guidance for activation of the spring
A-Decidous dentition period :

B-Early permanent dentition period :
1.Case of bony ankylosis of left T.M. Joint Physiotherapy after surgical intervention : For 4 Yrs. followed by orthodontic Treatment




2. Bony ankylosis of T.M. Joint under develop mandible

Appliance I in action

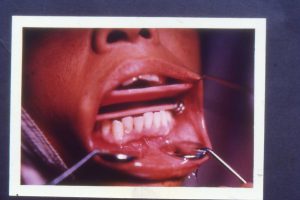
3. Bony ankylosis following trauma and condylar fracture
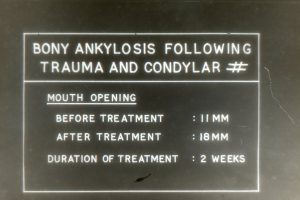
Initial mouth Opening

Physiotherapy with appliance
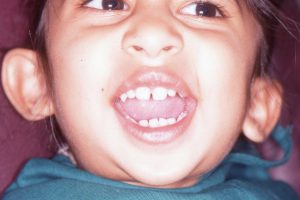
4. Fibrous Ankylosis of T.M. Joint
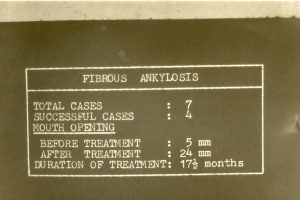
Initial Opening

With appliance 11

Opening achieved
5. Sub mucous Fibrosis Lesion in the cheek (before treatment)

After chemotherapy and physiotherapy

(Opening increased from 29mm to 36 mm)
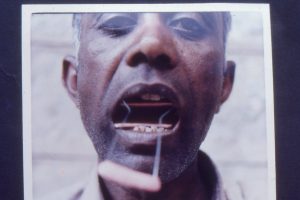
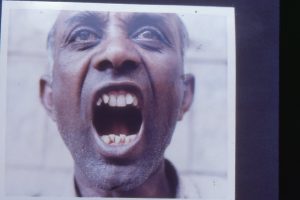
6. Myositis Ossificans (Anterior fibers of right masseter muscle)
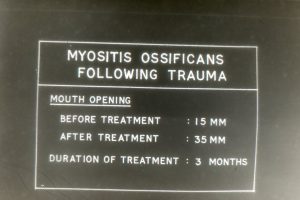
Mouth opening after surgical intervention

With appliance
After the treatment
7. Osteoarthritis of T.M. Jionts Initial opening 11 mm

Appliance in action (type1)

Appliance in action – opening

Opening achieved along with lateral movement (45mm)

8. oral trismus due to radiation : Initial opening

With appliance

After 6 months

A. Size of the appliance
It is good to make the appliance as per the size of the maxillary dental arch. When the patient can open the mouth to some extent, wax bite registration can be done ( fig of the patient with wax bite in the mouth).wax bite is trimmed leaving a margin of 2.0mm from the facial margin of the teeth.(Fig. wax bite trimming) . anteriorly wax bite is trimmed as shown in the picture (fig1) keeping the margin mesial to first premolars. (In case of deciduous dentition, the appliance is placed on first and second deciduous molars)(Fig –wax bite)
B. Selection of the wire
Wire used is stainless steel (orthodontic) wire, varying in the gauze from 0.9mm to 1.2mm depending upon the nature of trismus and age of the patient. The size of the coil may vary from 5.0mm to 10.0mm depending upon the nature of trismus and age of the patient.
C. Appliance can be fabricated as per the following illustration:

1. Measurement taken for the appliance size

2. Trimming of the waxbite

3. Waxbite of the required size
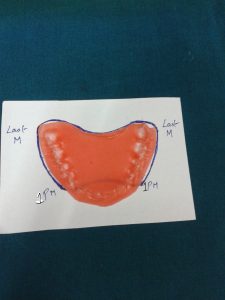
4. Waxbite size mark on the paper
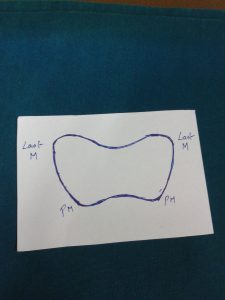
5. Size of the appliance to be made
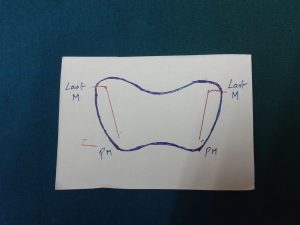
6. Position of the Mandibular springs
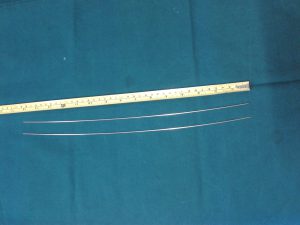
7. Length of the wire to be taken (30 to 35 cm)

8. Mandibular arm of the spring
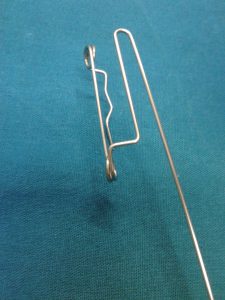
9. Spring completed with maxillary arm

10. Springs aligned on a glass slab as per the size taken


11. Arcylization of the appliance


12. Mandibular plat of the appliance made.


13. Process of acrylization

14. Making of maxillary plat of the spring

15. Spring completed with handle

16. Zigzag markings on the occlusive aspects of the appliance for better positioning of the appliance.

17. Blue dot’s used for measuring the activation of the springs.
“LET THE PEOPLE SMILE, ITS GOOD FOR HEALTH AND SOCIETY”
A RAY OF HOPE FOR THOSE WHO HAVE LOST IT
PROGRESS AND PEACE SHOULD GO TOGETHER.
© . All Rights Reserved